A few weeks ago we admitted Sylvia. She had been feeling unwell for a some days, with fever and episodes of uncontrollable shaking. What really alarmed her was when she turned yellow, and then developed abdominal pain and vomited a couple of times. Sylvia is forty eight, and had always been healthy. She rowed with the local club twice a week and kept her weight under control. For the past year or so she noticed that she got pains in her abdomen after eating fatty foods such as fish and chips, and now avoided foods like that. It was her son who noticed she was yellow – he then phoned Sylvia’s GP. The duty doctor came and confirmed that she was indeed jaundiced, feverish and unwell, and persuaded her that she needed to go to hospital.

We did all the usual things for someone with suspected biliary sepsis. Took blood cultures and routine blood tests. These tests confirmed she had elevated bilirubin and transaminases, increased alkaline phosphatase, as well as a high neutrophil count and CRP. We gave her intravenous fluids, anti-emetics and antibiotics. We were able to get an ultrasound within a couple of hours. Ultrasound is really good at looking at the liver and biliary system in jaundiced patients – better than CT.
The ultrasound showed that Sylvia had a gallbladder full of gallstones and her common bile duct was dilated. It seemed likely that she had a stone blocking the flow of bile from the liver to the duodenum, and that the stagnant bile had become infected with bacteria causing ascending cholangitis and liver inflammation.
The questions I want to answer this week are:
Why did Sylvia turn yellow?
What are gallstones made of and why do they form?
Why is there an increase in alkaline phosphatase in the bloodstream when the biliary system is obstructed?
The last of those questions is the hardest, but I will make some conjectures, and hope that others who know more about it will correct me.
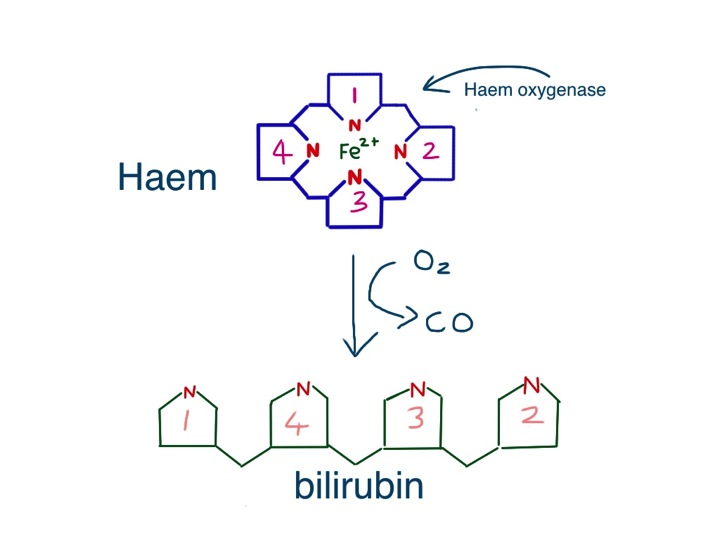
Jaundice is fairly straightforward. It is caused by the accumulation of bilirubin, which is a greenish-yellow colour. Bilirubin is made from haem, the central working part of myoglobin, but most bilirubin comes from the breakdown of haem in the haemoglobin from red blood cells.
So why is haemoglobin red? It is not only – or even mainly – the iron that makes haem red, but the porphorin ring that surrounds the iron. This large ring is made of four smaller pyrrole rings.
Pyrroles are often coloured – the dye indigo has two pyrrole rings and red acrylic paint often contains the dye pyrrole-red. Melanin, the pigment that gives skin and hair its colour is brown or black or red because it has a related structure – indole – a pyrrole stuck to a benzene ring. Without this pyrrole ring we would be like albinos, but without pink skin and eyes. As we shall see, we would also produce beige poo and colourless urine.

Red blood cells last on average 120 days before they wear out and have to be recycled. As we have five litres of blood and in each litre there is at least 120 grammes of haemoglobin, it means we have to make, and break down, five grammes a day. About a teaspoonful. This all happens inside macrophages in the spleen and liver, as they try to salvage useful parts of the red cells to make new things.
Macrophages are similar to neutrophils but slightly smarter. Some are good at host defence: they come to the scene after the neutrophils have done their job, do the forensics, and find out what the germs are made of. They then tell the lymphocytes how to make antibodies to protect us in the future.
Other macrophages are good at clearing up the mess, breaking down dead tissue and making things neat and clean. The spleen and liver macrophages that deal with old red cells are the latter kind. When they take red cells apart, they separate haem from globin, and then take the iron out of the haem. Next, the porphorin ring is broken to form bilirubin – its molecule of linked pyrrole rings looks like four beach huts in a row.
The bilirubin is then thrown away (I don’t know why it can’t be re-used). It attaches to albumin and becomes water soluble after conjugating in the liver with a sugary molecule called glucuronate. The conjugated bilirubin is then transported into the biliary system, stored in the gallbladder, and squirted into the duodenum when we eat fatty food. In the bowel, it is converted to urobilinogen, which makes poo brown. Some is reabsorbed and excreted in urine, which makes urine yellow.
Sylvia had noticed that her poo had changed colour – it had become putty-coloured – and her urine had become much darker. That is because conjugated bilirubin was not getting into her intestines and instead some had leaked into her bloodstream and was appearing in her urine. The whites of her eyes and skin had become yellow because of the very high level of conjugated bilirubin in her blood.
Now to the gallstones. In Western countries they are most commonly made of cholesterol. I have already talked about the importance of cholesterol in keeping cell membranes rigid and non-leaky. Cholesterol is made in large amounts by the liver and transported to other cells gift-wrapped as LDL cholesterol. It is also used to make bile salts. It only needs a minor modification of the basic chemical structure of cholesterol to make bile salts – the main component in bile which makes it work – the main function of bile salts is to help us digest dietary fat.
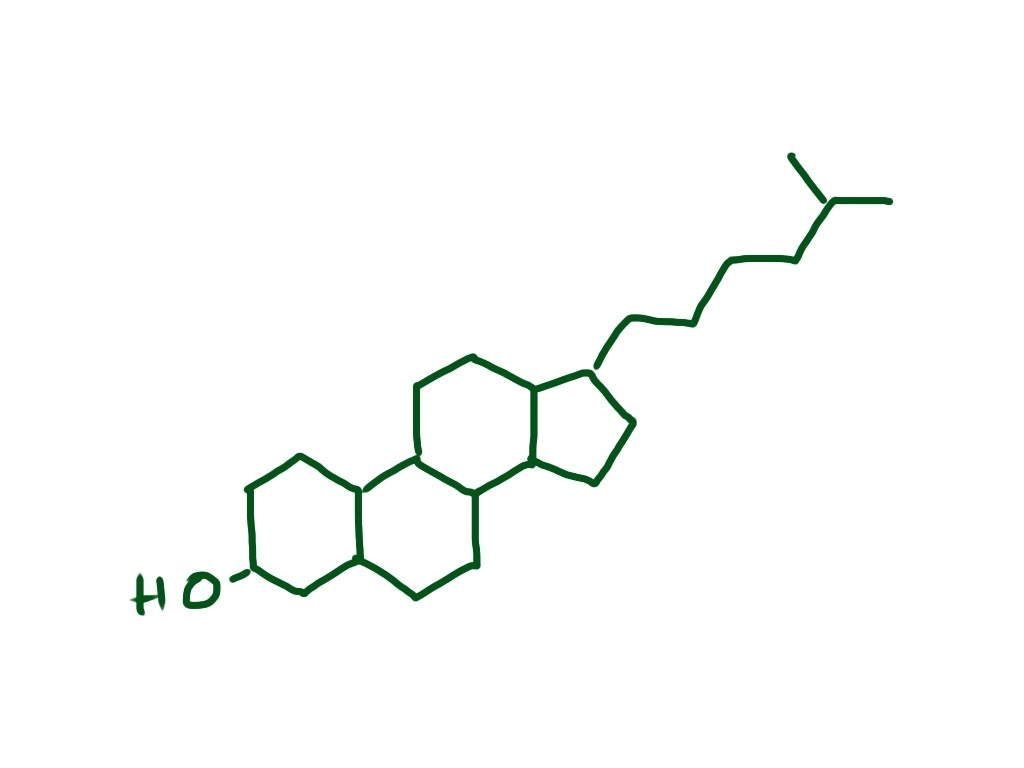
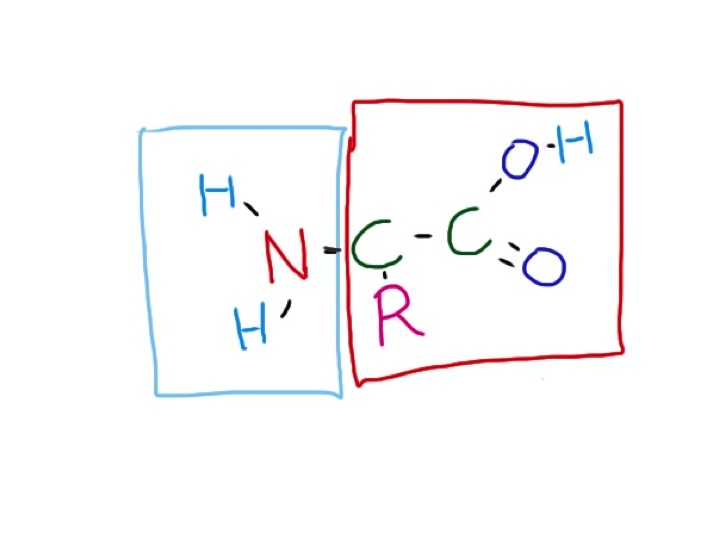
Bile salts are detergents. Just like washing-up liquid, they emulsify fats, breaking large fat globules into smaller micelles which do not stick to each other, or anything else. Cholesterol is essentially very insoluble in water, or hydrophobic. When an organic acid group is added – to make bile salts – it gains a hydrophilic or water-attracting group. This is just like soap – a long lipid chain with an organic acid group at the end. The hydrophobic lipid part is embedded in the tiny fat globule and the hydrophilic groups stick outside in the watery medium of the intestinal contents.

As well as bile salts, the liver secretes phospholipids into bile – principally phosphatidylcholine. This, with cholesterol, is the main stuff cell membranes are made of. It is also an emulsifying agent, and is used extensively in the food industry to keep fats in suspension.
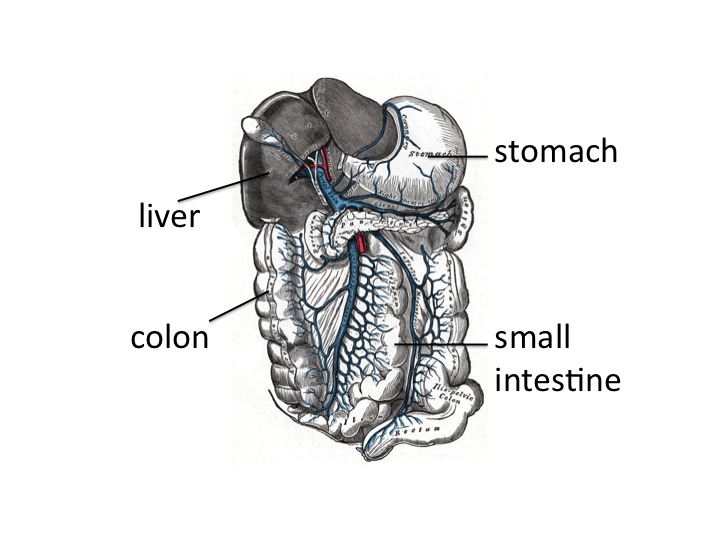
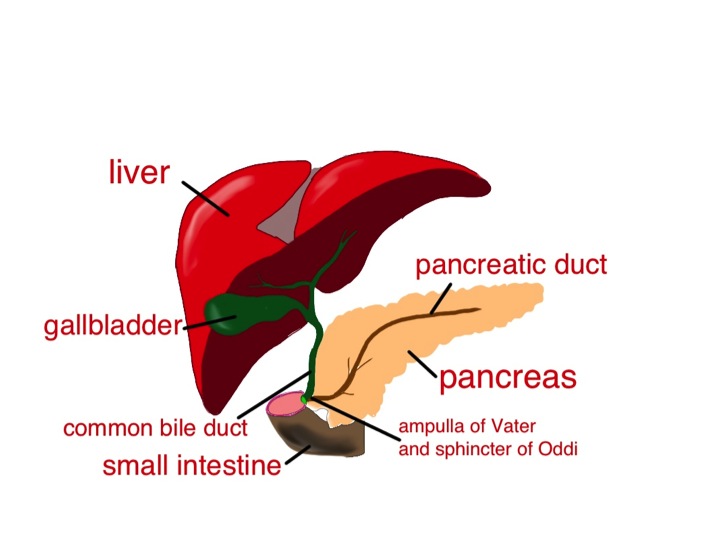
So, when we eat fat, the small intestine detects it and releases the hormone cholecystokinin (CCK). This causes the gallbladder to contract to send bile into the duodenum, and also makes the pancreas release enzymes, including lipase. CCK also has some very interesting effects on our brains, making us feel less hungry, and curiously, opposing the effects of opiate drugs. The bile and pancreatic secretions are both delivered into the duodenum through the same tube – see diagram. The detergent bile salts, emulsifying phospholipid and pancreatic lipase are designed to work together to digest fat.
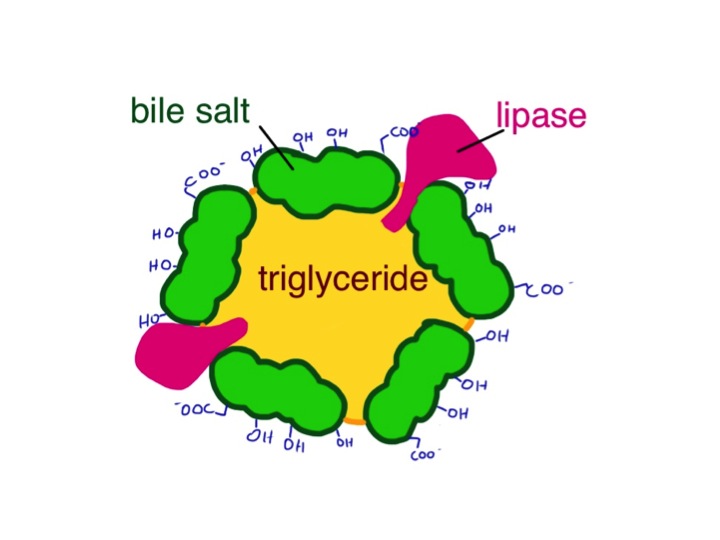
The bile breaks it up into tiny globules and the lipase breaks triglyceride into fatty acids and monoglyceride. These are transported across the intestinal mucosal cell membrane and then the triglyceride is put back together again. Seems a daft system, but it clearly works. The triglyceride is taken away from the intestine not in the portal blood, like most other substances absorbed by the gut, but in the lymphatic system in the form of chylomicrons – small fatty globules covered by a layer of phospholipid. The chylomicrons travel up the lymphatic vessels to emerge into the circulation just below our left clavicle. This means that it avoids passing straight away through the liver. If blood is taken soon after a fatty meal and centrifuged, it will have a milky appearance because of the large amount of chylomicrons.
So why do gallstones form? As well as bile salts, unmodified cholesterol is also secreted into bile. It is only kept soluble by the bile salts and phospholipid – the ratio of cholesterol to bile salts and phospholipid is therefore important. When it goes wrong, cholesterol precipitates out and forms solid stones like those that caused all Sylvia’s recent problems – a bit like when I try to make mayonnaise and it curdles – the fat becomes un-emulsified and separates out.
In some parts of the world, gallstones are made from bile pigment – bilirubin. This can be due to increased red blood cell breakdown resulting from abnormalities such as sickle cell disease, but it’s also common in East Asia, for reasons which are not clear. A good, comprehensive analysis of why gallstones of all types form can be found at:
http://gastro.ucsd.edu/fellowship/materials/Documents/Gallstones/pathogenesis%20gallstones.pdf
Now the alkaline phosphatase. Bile is alkaline. Alkaline phosphatase is an enzyme that removes phosphate groups in alkaline conditions. When bile flow is blocked – by stones, as in Sylvia’s case, or for any other reason – the liver makes much more alkaline phosphatase, some of which appears in the blood. Bones use a similar alkaline phosphatase to rearrange phosphate groups to make hydroxyapatite – the hard stuff bone is made from. Most of the alkaline phosphatase normally in our blood is the bone sort.
There is plenty of information about whether alkaline phosphatase is from bone or liver, but very little I can find that suggests why the liver should make this enzyme when the biliary system is blocked. I think a clue here is that neutrophils also have alkaline phosphatase in their granules, which help kill bacteria. This is in addition to the myeloperoxidase and esterase mentioned in earlier posts. Why should a phosphatase be damaging to bacteria? The answer may well involve techoic acid, an important reinforcing molecule in some gram-positive bacteria.
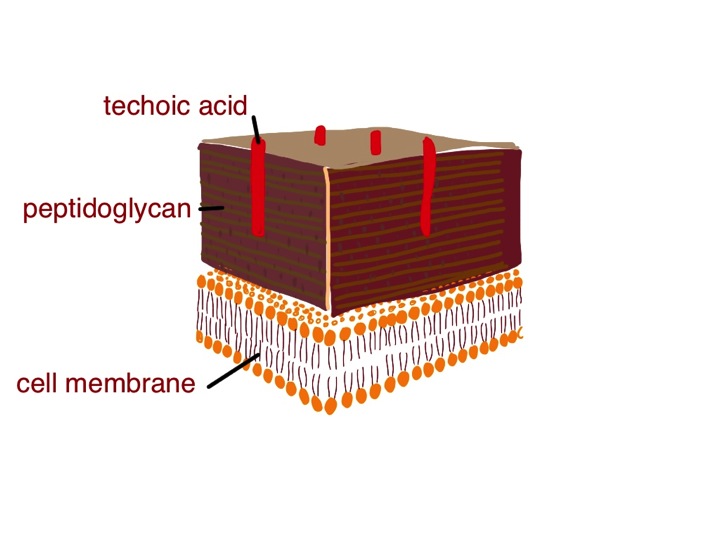
In these microbes, techoic acid strengthens the peptidoglycan cell wall and inhibits the action of lysozyme, yet another enzyme made by neutrophils. Lysozyme is designed to break some of the sugar-sugar bonds in peptidoglycan – so getting rid of the techoic acid would surely be helpful. We know that alkaline phosphatase is effective in breaking up techoic acid – see, for instance:
http://jb.asm.org/content/102/3/747.short
Maybe the liver is producing this anti-bacterial enzyme to help prevent infection when the flow of bile slows down. Unfortunately, this won’t work with gram negative organisms such as E.coli because they don’t make techoic acid – and it was a gram negative bacterium we grew from Sylvia’s blood culture – the germ that was causing her ascending cholangitis.
Soon after she came in, Sylvia had an ERCP – an endoscopic retrograde cholangio-pancreatoscopy. The endoscopist managed to remove the impacted gallstone from her ampulla of Vater, and she quickly recovered. A week later she had her gallbladder removed, including the stones, and now is quite well – she can even eat fish and chips.
Now to the food link: mayonnaise.

This is an emulsion of lipid, such as olive oil, in an aqueous (watery) medium – vinegar or lemon juice. The emulsifying agent is raw egg yolk, which – just like bile – contains lots of phospholipid – phophatidylcholine and is also rich in cholesterol. In France, mustard is also added. Mustard seed contains mucilage, a gooey stuff that some plants produce made of sugar polymers. (Thanks again to Harold McGee). These also act as emulsifiers and further thicken the mayonnaise, and give it a better taste. When I make cheese sauce, I use a sugar polymer (flour) to achieve a stable emulsion between butter and milk – no doubt the phospholipid in the milk helps too. It seems likely that in the small intestine, the mucus from the stomach, a similar gloopy sugar polymer, probably has a similar effect to mustard seed mucilage to help with fat emulsification.