We admit a lot of elderly patients who have fallen over. There are a whole range of problems which cause falls, one of which is postural, or orthostatic hypotension. Emily is 78 and lives alone in a bungalow. Her husband died three years ago, but her daughter calls in to help most days. She was fairly well until she went to her family doctor’s surgery last week and had her blood pressure measured. The result was not good – 186/88mmHg.
She first developed high blood pressure when she was in her fifties, and it had crept up since. She was already taking ramipril (an ACE inhibitor) and indapamide (a thiazide diuretic). She had tried amlodipine, but that gave her swollen ankles, which she hated. Her GP decided to try her on doxazosin. This is an alpha-blocker that lowers blood pressure by opening up small arteries. The morning of the day of admission she got up and took her tablets. Then she had a bath, but when she got out felt awful, and faint, and fell to the floor. She lay on the floor for a few minutes and tried to get up, but felt very dizzy and had to lie down again. She phoned her next-door neighbour on her mobile phone. The neighbour came round and helped Emily to her feet, but she went wobbly and could not stand, ending up on the floor again. Her neighbour became really worried and called for the ambulance. When the ambulance paramedics arrived they found that when they tried to stand Emily up, her blood pressure dropped from 160mmHg systolic to 90mmHg. They brought her in to see us.
There is a popular notion that all antihypertensive drugs cause postural hypotension, but this is not the case. As we will see, beta-blockers can even be used to treat this condition.
What is happening with the circulation to cause Emily’s blood pressure to drop when she stands up?
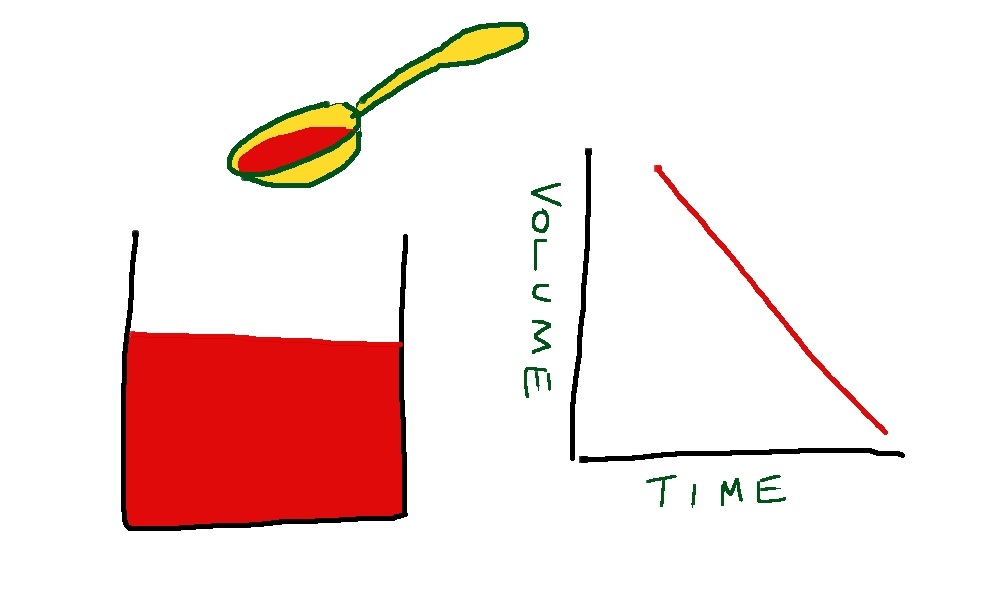
The whole explanation is made much easier with a standard hospital rubber glove (the stretchier the better) and a sink, and a supply of water. First we fill the glove up with the right amount of water.
The water in the glove represents blood in the venous side of the circulation. The arterial side is much lower volume, and is very little affected by changes in pressure due to posture.
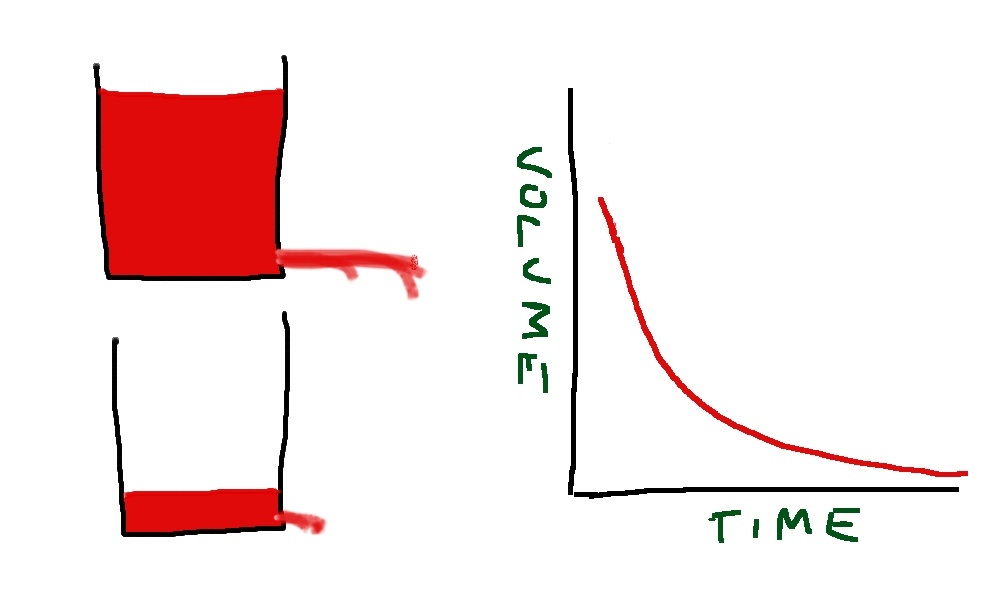
When we stand up the amount of fluid in the veins of the legs and abdomen increases, due to increase in hydrostatic pressure stretching the rubbery material. Veins are thin-walled and rubbery, and will naturally distend if the pressure inside is increased. If this happens, the thumb empties, this represents the filling pressure to the heart. If cardiac filling pressure drops, cardiac output drops and blood pressure falls.

This will result in a fall in systemic arterial blood pressure – postural hypotension.
But this does not happen in healthy, young people. We have autonomic reflexes which cause constriction of veins before we stand up, so that filling pressure to the heart is maintained. In the glove model this is represented by my hand squeezing the fingers and main hand of the glove.
There are two main causes for postural hypotension – failure of autonomic squeeze of the veins, and insufficient filling of the venous compartment.
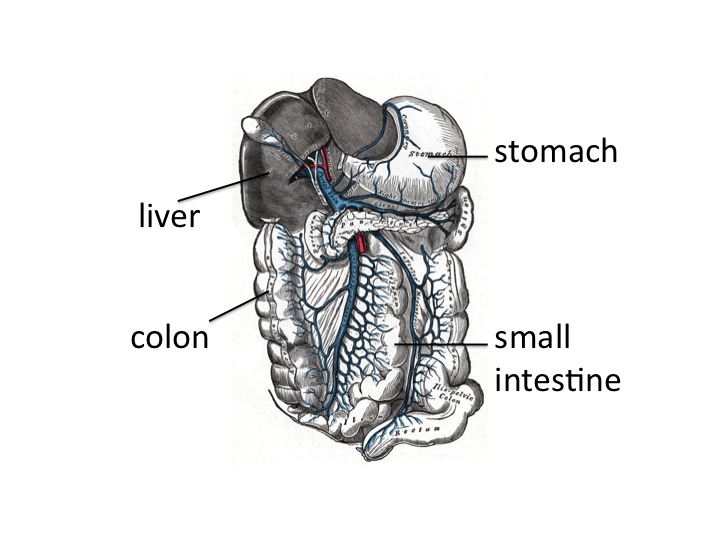
Let’s take the first of these – not enough squeeze. When we move from lying down to standing up, our brain knows what is about to happen. As we move our limbs the proprioceptors in our joints tell our brain what is about to happen and our conscious mind probably also has a role. Messages are sent to the control centre (Houston – prepare for lift-off) in the medulla. Sympathetic nerves send messages down to the veins to tell them to constrict. It is interesting that human intra-abdominal mesenteric veins are particularly richly supplied with sympathetic nerve endings – presumably because we are one of the few animals where standing is such a problem. In animals such as horses and dogs, moving from lying to standing does not involve a capacious venous network to be subjected to large pressure changes – their legs have very little venous blood and their abdomen and contents is on the same level as the heart.
It is also not surprising that if you take a healthy, young person and strap them to a tilt-table, and suddenly move them from horizontal to vertical, they will experience an impressive drop in blood pressure. If they are lying on a bed and stand up – blood pressure hardly changes because the brain-stem prepares us for the change in posture with messages to our abdominal and leg veins to constrict.
As we get older, everything starts to go wrong (see last week’s post). Autonomic reflexes become impaired. Patients with Parkinson’s disease are particularly prone to develop postural hypotension because of impaired brain stem autonomic reflexes – this used to be called Shy-Drager syndrome when I was young – it is now know as multi-system atrophy. Some drugs such as antidepressants and methydopa inhibit brain stem sympathetic output and predispose to this condition.
The sympathetic nerves end up on the outside (adventitia) of veins and release noradrenaline which causes constriction of venous smooth muscle by stimulating alpha receptors. Emily had been given an alpha-blocker to reduce constriction of her arterioles and thereby reduce blood pressure. In her it reduced the ability of veins to constrict when standing up by blocking venous alpha receptors.
Some patients have problems with the autonomic nerves. Diabetics and alcoholics are prone to develop autonomic neuropathy which may result in postural hypotension due to inability of veins to constrict.
Temperature also plays a part in venous constriction. Most of us have noticed occasionally when getting out of a hot bath or sauna feeling dizzy for a few seconds, we hold onto the edge of the bath then things improve. What has happened is that the hot bath water has caused venous dilatation and the normal reflexes have not been enough to maintain cardiac filling pressure. Cardiac output drops, baroreceptors panic (Houston, we have a problem). Houston responds quickly by sending a stronger sympathetic signal to the veins and to the heart to increase cardiac output and the problem is soon sorted. But of course preventing the problem is much better than reacting when it has happened.
The second main cause of postural hypotension is insufficient fluid in the circulation.

In Emily’s case this may have been partly due to the thiazide diuretic she was taking for her blood pressure. Patients on loop diuretics such as furosemide are even more prone to fluid depletion. Sepsis causes problems with a postural blood pressure drop because of fluid shifts out of the circulation into interstitial spaces, and because fever causes venous dilatation as in the hot bath above. Jonathan, who had a lobar pneumonia a few weeks ago, may well have collapsed in his GP’s surgery because of a postural blood pressure problem.
Blood loss from trauma or intestinal bleeding may often not result in blood pressure drop until the patient stands up – it is far easier to maintain filling pressure when lying down and not having to squeeze the veins hard.
Sorting out Emily’s postural hypotension was straightforward. We gave her two litres of intravenous saline and stopped her doxazosin, and diuretics. We had a plan to start her on verapamil or diltiazem when she could stand up without her blood pressure dropping – which it did the next day.
Do ACE inhibitors/ARBs, beta blockers or calcium channel blockers cause postural hypotension?
The answer is to begin with, no and no.
ACE inhibitors can cause a postural drop when they are first started. This is because angiotensin does have an effect on venous constriction, but only transiently when it is increased or decreased. If angiotensin II is infused into a hand vein it will constrict, but only for a few hours at most. Similarly if angiotensin II is withdrawn, the vein will dilate, but only briefly. This means that it is prudent to warn patients that they may develop postural symptoms following the first dose – and it is a good idea to take it when lying down before going to bed. The effect of angiotensin II on arterioles is long-lasting, which is why these drugs are useful in treating arterial hypertension.
Beta blockers reduce blood pressure by mechanisms which are not completely understood, but is likely to be a combination of reduced cardiac output and inhibition of renin release from the kidney. There are beta2 receptors in arteries and veins, but these cause vascular dilatation. Beta blockers can help veins constrict, which is why they are sometimes used to treat postural hypotension. Having said that, if there is a postural drop in blood pressure, the reflex mechanisms set in train by baroreceptors involve increased sympathetic stimulation to the heart via beta1 receptors, increasing force and rate of contraction. Beta blockers will block this response and may therefore impair the recovery from an episode of postural hypotension, but they will not cause it.
Calcium channel blockers have an effect on arterioles, not on veins. Calcium channels are important in maintaining arterial tone, but not venous tone. Venous tone depends almost entirely on sympathetic stimulation. Therefore, at least in theory, drugs such as verapamil, diltiazem and amlodipine will not cause a postural drop. But of course if there is a postural drop, lower initial blood pressure caused by these agents may make the episode worse.
Sorting out Emily’s orthostatic hypotension was fairly straightforward. What about when it is caused by age-related impairment of brain stem function, or by irreversible peripheral autonomic neuropathy? It can be a real problem.

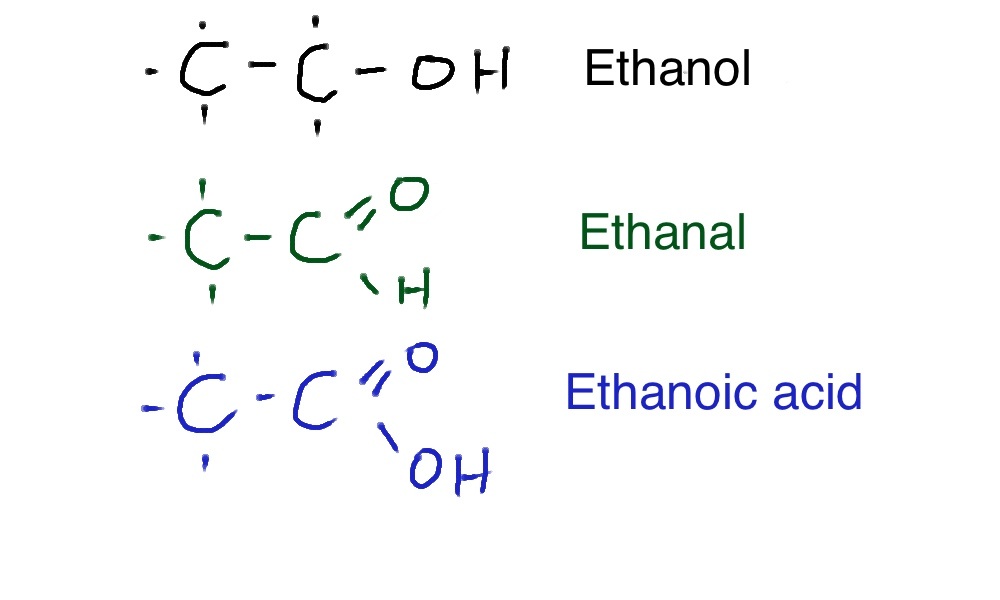
One approach is to use fludrocortisone. This is a synthetic analogue of aldosterone. Made from cholesterol (again!) this hormone is made in the adrenal cortex, in different cells which make cortisol from cholesterol. The function of aldosterone is to regulate how much salt and water is excreted from our kidneys. Aldosterone helps the reabsorption of more salt from the distal convoluted tubule and will therefore increase circulating volume of blood. This will have the opposite effect to diuretics and overfill the circulation and help keep filling pressure at heart level adequate on standing up. Another drug which is sometimes used is midodrine, an alpha receptor agonist, helping constrict veins and maintain cardiac filling when upright. The drug does not have a licence for this indication in the UK.
We have made a not very good video showing how postural hypotension works – my first attempt at youtube – thanks for your help Steph. We will try to make a better one soon and update this post. The video is at:
The food link this week was not obvious when I started, but of course it has to be liquorice.

Liquorice contains glycyrrhizin which has a chemical structure similar to steroids such as cholesterol and aldosterone (made from cholesterol – again!). It has long been known to have a mineralocorticoid effect. This is not because it acts directly in the kidney to stimulate aldosterone receptors. Instead it prevents the conversion of cortisol to cortisone. Cortisone, synthesized by the adrenal glands, is converted to cortisol in the kidney, then back to cortisone, cortisol has more mineralocorticosteroid effects than cortisone – full details are in the NEJM paper:
http://www.nejm.org/doi/full/10.1056/NEJM199110243251706
Eating too much liquorice can cause high blood pressure and low plasma potassium levels – similar to primary hyperaldosteronism.