Robbie was really happy to be diagnosed with pulmonary tuberculosis. Before he arrived he was convinced he had lung cancer.
Robbie is in his late 50’s, he was born in Glasgow and left school at fifteen with no qualifications. His father was a shipbuilder on the Clyde. Robbie thought he would do the same, but in the seventies the shipyards closed* and there were no prospects for young men like him, so he came south.
He got various unskilled jobs, mainly in the china clay industry, got married and had two daughters. But he drank much too much and was not faithful to his wife, who left him. He says he does not entirely regret it – he had a great time.
Or as George Best famously said “I spent a lot of money on booze, birds and fast cars, the rest I just squandered”

Then, about three months ago, he developed a cough that kept him up at night. He had terrible sweats and would wake up in the morning with his bedclothes really wet. He took the sheets off his bed to hang them up to dry during the day. He knew something was seriously wrong when he started coughing up blood and was losing a lot of weight. He had always been “wiry” but now was becoming skeletal. Robbie became increasingly sure he had lung cancer, but was too frightened to get help. He still talked to his daughters every Sunday on the ‘phone. Last Sunday one of them was so worried when he told her what was happening that she went to find him and brought him in to our hospital. He had a chest Xray and within a couple of hours we told him that we thought he might have TB.

We put him in a side-room and got him to cough up some blood-stained sputum which we sent to the lab. Within a couple more hours we got a phone call to say that the sample was “teeming” with AFBs – acid-fast bacilli.
I have previously talked about bacterial cell walls and the Gram stain, which is a process which involves staining a biological sampe with a blue and red stain which have different affinities for the various components of a bacterial cell wall. Gram-positive bacteria stain bluish-purple with this stain because their cell wall is mainly peptidoglycan. Gram-negative have a thin layer of peptidoglycan, but a thick covering layer of lipopolysaccharide (LPS), which, like peptidoglycan, helps protect the germ from damage. As its name suggests, LPS is made of chains of sugar molecules and lipids – with carbon chains about 16-20 carbon atoms – similar to those in triglycerides in butter and olive oil. Gram-negative bacteria look red under the microscope after the Gram staining process
Tuberculosis is caused by the bacterium mycobacterium tuberculosis. It has a quite different cell wall structure which makes it very difficult for our white cells to destroy. The secret weapon is mycolic acid. This a long molecule composed mainly of hydrocarbon chains – up to 54 carbon atoms long.
Hydrocarbon chains are common in all sorts of lengths in nature, most of which are useful to us. One carbon atom, surrounded by four hydrogen atoms is methane – a gas which I rely on to cook my dinner. Three or four carbons and we get the gases propane and butane, also useful in cooking the barbecue. Octane, a liquid with eight carbon atoms gets me to work in the morning. When we get to 16-20 carbon atoms there are endless things I can get from the supermarket, mainly to eat, with this size of hydrocarbon chain. These are mainly liquids or soft solids such as olive oil, butter, meat fat, and cooking oil. With longer hydrocarbon chains we are talking about waxes. Waxes have huge numbers of use in nature and are used extensively by humans, but mainly for protection rather than as a food. We use waxes a lot for protection – shoe and furniture polish for instance.

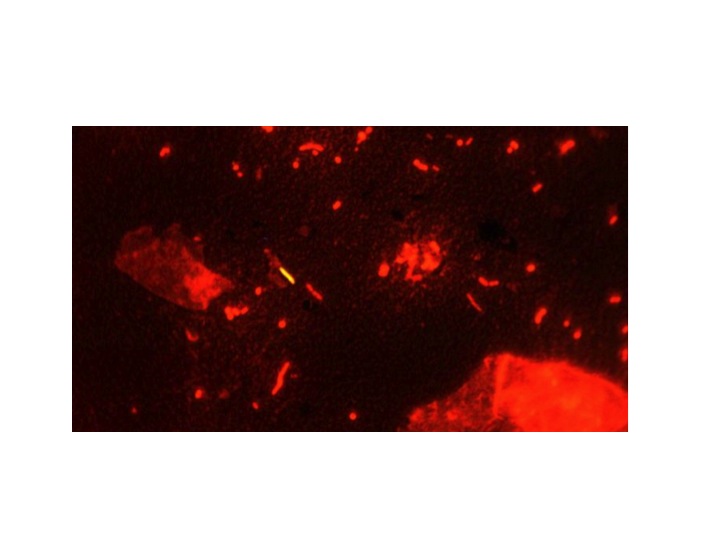
The wax in our ears is a mixture of squalene, a hydrocarbon of 26 carbon atoms mixed with cholesterol and dead skin cells, also designed to protect us from microbial infection. Plants produce waxes to protect the surface of their leaves, and sheep produce waxes to protect their wool (lanolin, chemically similar to earwax). Waxes are protective because they are difficult to break down chemically. The tuberculosis bacteria use this property of wax to protect them from the nasty chemicals white blood cells use to try to destroy them. We can detect mycobacteria by using a special stain which is taken up by the waxy coating. The original stain was called Ziehl–Neelsen, or ZN, but we now use a better one called auramine. This is a fluorescent dye which sticks to the wax, even when the specimen is flooded with acid and alcohol, which will remove it from just about any other bacteria which do not have mycolic acid in their cell wall. The specimen is then viewed under ultraviolet light and the TB germs light up.
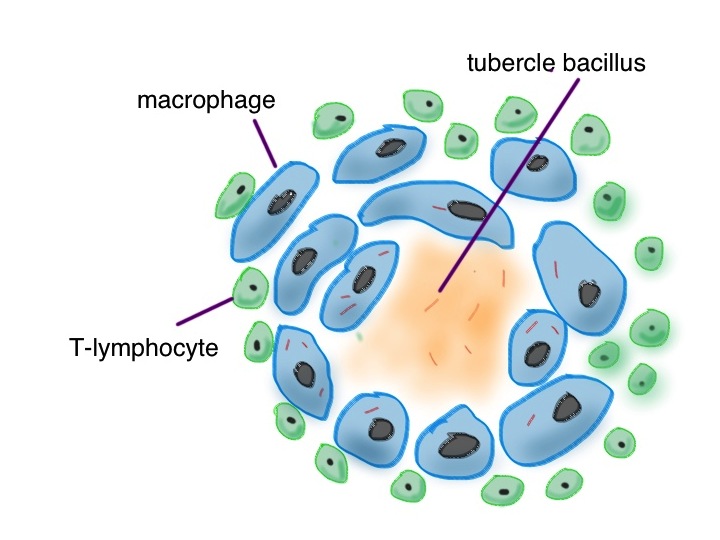
Pulmonary TB is transmitted from one human to another mainly by coughing – producing a fine spray of droplets which contain the tuberculosis bacteria. Robbie mixed with a number of alcoholics and drug addicts, who are more prone to develop this disease. When the bacteria are detected by the cells lining the lung (see asthma and pineapple below), neutrophils will have a go at engulfing them and soaking them with lysozyme and bleach. TB germs will laugh at that (no, not really, TB germs don’t have much of a sense of humour). Their waxy coat makes them impervious to hypochlorite. Then the professionals are called in –macrophages. They will also engulf the tubercle bacilli. They will then call in help from T-lymphocytes, walling off the tubercle germs in a special structure called a granuloma.
The TB germs can only grow very slowly, because they have to make the very long hydrocarbon chains to protect the new bacterium after cell division. Macrophages and lymphocytes use all the weapons at their disposal to try to kill them, many of which I think we don’t properly understand. We do know that nitric oxide, made by neutrophils is important. This is a gas which can penetrate the waxy coat and damage the TB germs. Another important molecule is thought to be granulysin made by cytotoxic T-cells. We don’t know how either of these molecules really do the damage and kill TB. Usually the human wins, but in about one in ten, as in Robbie’s case, TB wins. Robbie’s smoking and previous exposure to clay dust will have caused lung damage, which makes him more susceptible. His heavy drinking and poor diet will also make it worse. Some think vitamin D, which is made in the skin from cholesterol and sunlight might be important in defence against TB. Robbie likes dim, smoky rooms and avoids sunlight most of the time. Before effective drug therapy, sanitoriums would encourage patients to sit in balconies in the sun as part of their therapy, making lots of vitamin D.
Even when the human wins, it is not always a total victory. Sometimes there is an impasse, where the TB germs cannot be killed, but only constrained in the granuloma. In this siege scenario macrophages have another trick up their sleeve – calcification. Macrophages are very closely related to cells which make bone – osteoblasts. When the granuloma cannot be sterilised the macrophages start laying down insoluble calcium salts and imprison the TB germs. Often we see white spots on the chest xrays of elderly people who were exposed to TB when they were young – this is due to the TB calcium prisons which allowed their lungs to solve the problem of what to do with indestructible organisms.
It is quite likely that Robbie will recover from his TB, as long as he takes his drug therapy regularly, even though his lungs will end up even more damaged than they were. There are some very drug-resistant strains of TB emerging in India and Africa, but at present most TB in the UK is sensitive to rifampicin, isoniazid and ethambutol. He has promised his daughter that he will stop smoking and drinking so much, and eat better food.
This week’s food link is Edam cheese.

This is traditionally encased in a wax coating to protect it from drying out and from microbial spoilage. I do not really understand why micro-organisms have not yet worked out how to easily break down wax and use its energy for their benefit. It has the same calorific value as fat but is clearly unappetising for all the normal germs in my kitchen which are happy to feed on shorter chain hydrocarbons.
*There is a very powerful speech by Jimmy Reid, a Glasgow shipyard worker who was elected Rector of Glasgow University.
“The greatest speech since President Lincoln‘s Gettysburg Address”
– required reading:

![Campylobacter are helical, like H pylori - it helps them swim through the mucus layer and invade into the intestinal epithelium By De Wood, Pooley, USDA, ARS, EMU. [Public domain], via Wikimedia Commons](https://wardroundstuff.com/wp-content/uploads/2013/12/slide13.jpg)