This is the third in a series of rigors. Some doctors call them chills, but I think of a rigor as a really uncontrollable shaking episode. I remember when I was a junior surgical house officer I was looking after patients who had undergone prostate surgery. From the nursing station at one end of the ward, I would hear a bed shaking at the other end. The beds in those days had metal frames and really clanked loudly when someone had a rigor – which on the urology ward was due to gram-negative septicaemia.
“Could you please draw up some gentamicin and ampicillin?” I would ask the nurse as I walked down the ward, armed with blood culture bottles to see an elderly man looking very alarmed, shaky and unwell. I think these days we are more careful to make sure our patients do not have infected urine before operating on them.
Earlier this week we admitted Jonathan. A very fit 36 year-old man who had never been in hospital before, apart from when he had an arthroscopy for a damaged knee following a football injury. It started with him feeling off-colour, off his food, and generally aching all over. He thought he had the ‘flu. He woke up at four in the morning to find it really hurt on the left side of his chest when he tried to breathe deeply. He had never experienced pain like it before, even after the arthroscopy. Then he started shaking uncontrollably. He then began coughing, and that was even more painful. Then he coughed up some brownish-reddish, rusty-coloured dark phlegm. He got up and took some paracetamol, went back to bed, but could not sleep. He decided he could not go to work and went instead to his GPs surgery. He had another rigor while in the waiting room, stood up and collapsed to the floor. The practice nurse found a couch so he could lie down, and got the GP to see him straight away. He was with us a couple of hours later. By the time we got to see him he had had a chest X-ray which showed a left lower lobar pneumonia.
Pyelonephritis, ascending cholangitis and lobar pneumonia are the diseases which commonly cause severe rigors. Malaria is another we see less commonly in our part of the UK, but can certainly also produce impressive rigors. To get rigors you need to have a flood of microbes released over a short period of time, which happens if you have an organ such as the kidney, liver or lung full of germs. Other infections cause fever, but less commonly rigors.
The reason for shaking with rigors is that our body is trying to increase our temperature quickly. The mechanism is similar to shivering when we are cold – using muscle contraction to generate heat. Substances on the bacterial cell wall are recognised by Toll-like receptors on macrophages. This is part of the innate immune system which is designed to respond to a whole variety of germs. Toll-like receptors are on a range of white blood cells, intestinal epithelial cells, respiratory epithelial cells and vascular endothelium – all the places we need to keep a close eye on where the enemy is likely to invade. Lipopolysaccharide, the coating of gram-negative germs is the classic trigger. Techoic acid on the surface of gram positive organisms (see last week’s post) is another. These receptors can even recognise DNA sequences only found in bacterial but not in mammalian cells. When macrophages are alerted to the presence of bacteria, they generate cytokines such as interleukin 1 which circulate and are sensed by the hypothalamus in the brain. The hypothalamus is the part of the brain which regulates body temperature and coordinates the shaking response. When Jonathan started shaking he felt really cold, even though his body temperature was higher than normal. When we saw him in the emergency department he was wrapped in three blankets, even though it is always warm in there.
Why do we develop a fever with infections? There is some evidence that some bacteria such as Salmonella typhi, which causes typhoid fever, are less able to survive at 40 degrees than 37 degrees. Not sure it helps much with other germs.
The junior doctor took the history and examined Jonathan. He took blood cultures and prescribed intravenous co-amoxyclav and clarithromycin.
Making a diagnosis of lobar pneumonia is usually easy in hospital, when we have an X-ray to look at, although in the early stages the changes can be quite difficult to see. We are all taught as medical students what clinical signs to look for. I thought it would be useful to think about why they happen in patients with lung problems, and particularly pneumonia.
First it is worth thinking what the lungs are for. They do two main things: 1) get oxygen into our bloodstream from the air and 2) remove carbon dioxide from our blood so we can breathe it out. What happens when these vital functions don’t work properly? Normally our lungs are very good at getting oxygen into our bloodstream. Blood coming out of our lungs into the pulmonary vein and then into our main systemic arteries is usually saturated to 98%. We can measure this easily with a pulse oximeter. This is a wonderful device which has revolutionised our management of patients with respiratory conditions. It was invented in 1972 by Japanese engineers called Takuo Aoyagi and Michio Kishi. The way it works is that it shines two beams of light through the finger tip or earlobe. One beam is red light at wavelength about 610nm, the other is in the near infra-red at 910nm.
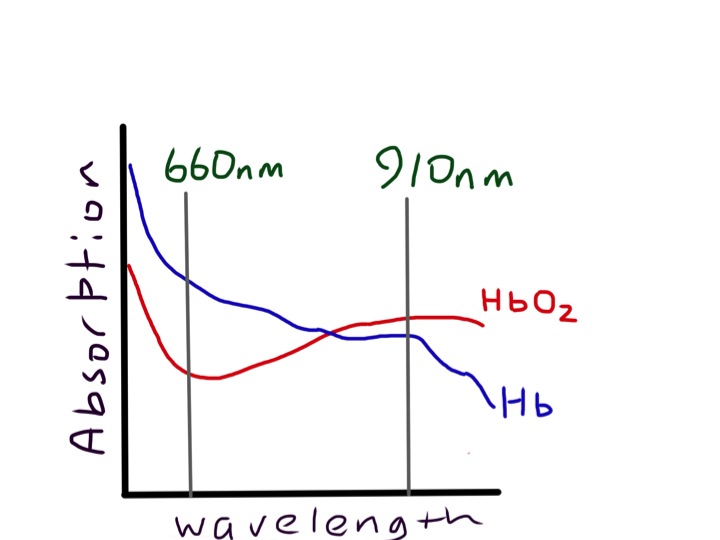
If you look at a pulse oximeter you can only see one red light, the infra-red is not visible.
Measurement of oxygen saturation relies on the absorbance of oxyhaemoglobin being different from deoxyhaemoglobin. We are talking about the colours of haem and pyrroles – again! Oxygenated arterial blood is well known to be redder than venous desaturated blood. The diagram shows that the absorbance spectrum of haemoglobin is very different at 610nm in the two types of haemoglobin. But at 900nm it is very similar. The machine compares the absorbance at the two wavelengths and can calculate the percent oxyhaemoglobin to deoxyhaemoglobin.

If it just did that, we would find that the haemoglobin in a fingertip is normally about 70% saturated, because most of the blood is in veins, rather than arteries. The really clever thing about a pulse oximeter is that it analyses the ratio of oxy- to deoxyhaemoglobin just in the pulsatile part of the signal. As the pulsatile part is due to arterial filling of the fingertip, this gives arterial, rather than venous oxygen saturation. Jonathan’s arterial saturation was 91% before he was given oxygen therapy, when it rose to 98%. There is a common misconception that hypoxia will make you breathless. Chemoreceptors in the carotid body and brain stem can certainly respond to hypoxia, but only when it is very reduced. Flying at 30,000 feet in a jet plane is equivalent to being at 8,000feet altitude where the oxygen tension is reduced by about 20%. Passengers in jet planes will often have oxygen saturations around 92% but do not feel breathless. In fact hypoxia does not cause breathlessness unless it is really marked. Why is this? – The reason is probably because increasing the rate of breathing does not help. Without oxygen, if I asked Jonathan to breathe faster, firstly he would find it difficult because it was so painful, but even if he did, his oxygen saturation would not improve. This is because there is shunting of blood in the part of his lung affected by the pneumonia. In the inflamed part of the lung there is increased blood flow, but the air spaces are full of pus. There is consolidation. Any blood which flows through this part of the lung will not be oxygenated and will emerge into the pulmonary vein desaturated. Even if the rest of the lung is working perfectly, saturating the blood to 100%, there is no way to resaturate the desaturated blood which has travelled through the abnormal lung, so his sats meter will detect this and show a low reading. It looks like evolution has sussed this out and doesn’t bother to make us breathe harder – unless the oxygen saturation drops to the mid 80s when various tissues in our body start to complain and generate lactic acid.
Carbon dioxide is a different story. Every day we breathe out about one kilo or two pounds of carbon dioxide. Our lungs are not designed to get rid of CO2 completely. Jonathan’s blood gas analysis showed a normal pCO2 of 5KPa (normal range 3.5-6). We need a certain amount of carbon dioxide in our blood to keep the acidity normal. But most (80%) of the carbon dioxide is in the form of bicarbonate (HCO3), made from carbon dioxide by the enzyme carbonic anhydrase in red blood cells.

If our lungs are not working, then carbon dioxide levels in the blood increase, bicarbonate increases, and hydrogen ion concentration increases, because of the balance between carbon dioxide and bicarbonate (see equation). We are all familiar with the reaction of bicarbonate and acid (vinegar or lemon juice) to produce carbon dioxide.

This is a reversible equilibrium reacation and in blood this can work the other way round so carbon dioxide makes acid and bicarbonate. This is known as respiratory acidosis. Unlike oxygen, our body is very sensitive to carbon dioxide levels. This is first detected in the carotid body, located at the division of the common carotid artery into internal and external branches, either side of the thyroid cartilage. This acts as an “early warning” signal, sending messages to the brain stem that
something is amiss and the lungs aren’t working properly. A few seconds later blood reaches the medulla in the brain stem, which is the central control mechanism for breathing, next to the vasomotor centre controlling the circulation. High carbon dioxide also stimulates the medulla, which sends messages to increase the rate and depth of breathing. Very soon the level of carbon dioxide is back to normal, but at the expense of a higher respiratory rate.
So back to Jonathan, he is mildly hypoxic, shown by low oxygen saturations, and has an increased respiratory rate at 28/min (normally less than 20/min). His lungs are not doing either of the things they are meant to do properly, take in oxygen or get rid of carbon dioxide. Oxygen saturation and respiratory rate are therefore the most important things to look at if you are worried about lung function. If they are normal, it’s likely that the lungs are working normally.
The next thing is chest expansion. What makes the chest wall move outwards when we breathe in? In healthy people sitting quietly, the chest wall hardly moves at all, because breathing is done by the diaphragm, acting like a bellows. Next time you are sitting next to someone in a lecture or watching television, look at their chest and you will see what I mean (I suggest you take care not to make it too obvious – sometimes scientific enquiry can be misinterpreted). When the diaphragm contracts it makes the abdominal wall move outwards. Jonathan’s chest was very obviously moving with each breath, although you could easily see that the left side moved less than the right – it is always the abnormal side which moves less. The chest moves outwards because the ribs are being pulled upwards by intercostal muscles pulling the ribs together. The whole rib cage moves upwards like a venetian blind being opened. The reason the ribs then move outwards is because of the way they are joined to the spine and sternum.

Like a bucket handle – if you pull it up it must move outwards. The outward movement increases the volume of the thoracic cavity and pulls air into the lungs. Jonathan is consciously stopping his left chest wall expanding – the inflamed pleural surfaces are rubbing together with each breath making it very painful.
I hope it’s clear that you can find an awful lot about a patient’s lung function without touching them. But all our doctors wear stethescopes around their necks, and it would be a shame not to use them. Before using the tubes, we can do useful things with our hands.

First of all percussion. This is pretty straightforward. It takes a bit of practice but it is certainly useful to tell if there is a pleural effusion or consolidation. In Jonathan, who is thin, it was quite easy to tell that the percussion note was duller over his left lower chest at the back.
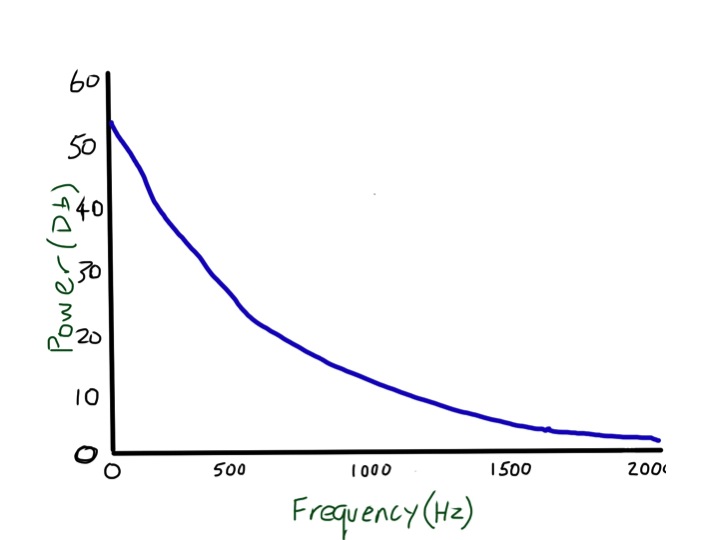
Then there is tactile vocal fremitus. Most non-respiratory doctors and students I have met seem to think this is something that is only worth doing in exams, and is an inferior test to listening with a stethoscope. This is not true. Testing tactile vocal fremitus involves putting your hands on the surface of the chest and asking the patient to say something and feeling whether the vibration can be felt with the palm or edge of the hand. In the UK doctors usually ask patients to say “ninety-nine”. Why ninety-nine? It comes from German physicians who realised that they needed the patients to say something with lots of low frequency sounds – “neunundneunzig” – the German for ninety-nine works very well. Ninety-nine in English doesn’t. I tried for a while getting patients to say “doom and gloom” but then one of the nurses took me aside and started asking about whether there was something I needed to talk about. At the suggestion of my wife, I am now trying “blue balloon” – seems to work pretty well. Why do we need a low frequency to feel the vibrations through the chest? I suggest you try an experiment – ask a good friend to you put your hands over his/her chest while she/he hums a note, starting low and slowly rising. If your friend is thin, the low notes will be easy to feel, but the buzzing feeling will disappear as soon as the note gets a bit higher. The frequency of a deep voice is about 150 cycles/second or 150Hz (middle C is 260Hz). The wavelength of that sound can be easily estimated – sound travels about 300 metres/second in air so that sound wave is about 2 metres long (of course you remember from school physics that the wavelength is equal to speed/frequency). When I calculated this I was surprised – I always thought that the wavelength of sound waves was tiny. In normal lung, these large wavelength noises are transmitted very easily, but when the note gets above 200Hz there is rapid attenuation, and at 2000Hz almost no sound gets through at all. That, and the fact that it is more difficult for hands to sense higher frequencies, mean that tactile vocal fremitus is better felt with lower frequencies.
These large, low frequency waves don’t get absorbed much by normal lung, but will be blocked if there is an air/fluid interface such as a pleural effusion. That means that tactile vocal fremitus is reduced or absent when there is fluid in the pleural space and can in fact be very useful for detecting quite small effusions. It is less useful in obese people because the fat overlying the chest wall is essentially fluid (see previous post about chest pain and haggis), and has a similar effect to pleural fluid. If you read textbooks about lung examination there is the suggestion that tactile vocal fremitus is increased over consolidated lung, such as in Jonathan’s case when he had a pneumonia. When we examined him he clearly had reduced tactile vocal fremitus at the bottom of his left lung, no doubt because the inflammation was associated with a small amount of fluid in the pleural space. I am not sure it is worth testing for fremitus anywhere apart from the lung bases, as it is only really good for looking for pleural effusions – but it is very good for doing that and should be routinely tested. If you disagree with this let me know – happy to host a discussion.
For more info see:
http://journal.publications.chestnet.org/data/Journals/CHEST/21004/399.pdf
Next we come to vocal resonance. Listening over the chest wall while the patient says something. I usually ask them to say “Mary had a little lamb”. If you have a stethoscope try listening to a friend’s chest while they say this. If they have normal lungs it will sound strange – really muffled – more like mooohoodloodleloom. If you put the stethoscope on their forehead it will not be distorted. Why does normal voice become distorted when heard with the stethoscope applied to the chest in people with normal lungs? It is because the high frequency bits of the voice are lost. Linguists call the high frequency sounds plosives – the sounds we make with our voices which involve our tongue stopping the flow of air to create t or d or c sounds. These are high frequency, well over 200Hz and are filtered out when travelling through normal lung. Why does normal lung filter out higher frequencies – that is more difficult, and needs an understanding of the physics of sound transmission through foams. If you want to read more I suggest you start with:
http://www.atsjournals.org/doi/pdf/10.1164/ajrccm.156.3.9701115
The left lower lobe of Jonathan’s lung was consolidated – filled with pus – fluid and neutrophils. Angry neutrophils making bleach and causing a lot of collateral damage to lung tissue and blood vessels. The hypochlorite bleach will rapidly oxidise haemoglobin to methaemoglobin (see long lie and salami below) to produce the characteristic rusty-red sputum he was coughing up. Because the lung is no longer like a foam, containing little air, high frequency sound travels much more easily and “Mary had a little lamb” is no longer distorted as in normal lung. This phenomenon, where voice is heard faithfully over consolidated lung is also known as bronchophony.
Similarly normal breath sounds are altered over consolidated lung. When our lungs are healthy, and we are at rest, air flows into our lungs in a laminar fashion, and makes very little noise.

When the speed of air increases beyond a critical value, the airflow becomes turbulent. This makes it noisy. Somewhat like when water is run into a bathtub – slow flow gives a clear, almost noiseless flow. When the tap is turned on more the water comes out in a noisy, bubbly flow. But turbulence in airways is useful – it mixes up gas more to improve delivery of oxygen and removal of carbon dioxide. Why not have turbulent breathing all the time? – well for one we would not like to sound like Darth Vader all the time, and it probably would not be the best thing for hunter-gatherer man when staying quiet was probably quite important for survival.
When we are running away from the hungry tiger a bit of noisy breathless breathing is probably not too much of a problem if it gives us better lung function. Turbulence causes a noise which has a hissing quality and has a whole range of frequencies from low to high – white noise. In normal lung the high frequencies are filtered out leaving a more muted sound (?pink noise) when heard on the chest wall – this is commonly described as vesicular breath sounds. When the high frequencies are also transmitted in consolidated lung the sound is harsher – bronchial breathing. If you want to hear what bronchial breathing sounds like put a stethoscope over that friend’s forehead while they take a deep breath in and out – the sound is not as loud as over the trachea but is not distorted. Whispering pectoriloquy is useful to confirm consolidation. We asked Jonathan to whisper “ninety-nine”. Whispered voice does not have any low frequency so cannot be heard well over normal lung. It could be heard clearly over clearly over his consolidated lung.
I could talk about other lung sounds such as crackles and wheezes, but this post has already become too long – maybe another time.
The next day Jonathan was much better, we grew a pneumococcus from his blood culture and he went home after two days on oral penicillin-based antibiotics.
The food link this week is scones.
I love scones, especially with jam and clotted cream and a nice cup of tea. They are traditionally made with sour milk and bicarbonate to make them rise in the oven. Milk goes sour when the lactose sugars are converted to lactic acid by lactobacilli. This lactic acid reacts at high temperature with the bicarbonate to make carbon dioxide gas that puffs up the scone to make it light and fluffy. This is the reverse of the reaction in our body when too much carbon dioxide turns into bicarbonate and acid (respiratory acidosis).
